EMR: Its Time Has Come
You are finally ready for EMR. Will you need a new practice management system, too?
BY JERRY HELZNER, SENIOR EDITOR
The history of EMR systems being used in ophthalmology practices dates back to the mid-1980s. However, when three highly touted systems launched bywell-respected healthcare companies failed to live up to expectations and were later withdrawn from the market, those in ophthalmology practices became wary of EMR and the market for such systems almost completely evaporated.
Until now.
Within the past year, a combination of factors has rekindled the interest of ophthalmology practices in EMR. These factors include the recent availability of more advanced EMR technology that can link to electronic practice management (sometimes called EPM) systems used for billing and scheduling, the implementation of HIPAA regulations, increasing pressure from third-party payers for practices to "go electronic," and possibly most important, the potential for achieving numerous efficiencies that translate to more dollars on the bottom line. These efficiencies can be more easily achieved by larger practices, though industry experts say that smaller practices should not ignore the potential benefits that can be derived from EMR. For example, it costs a practice using paper records an estimated overall cost of $3 to $6 to pull a chart. With EMR, that cost is virtually eliminated. "Ophthalmologists have been thinking about installing EMR for 10 years," says Jim Messier, vice president, Ophthalmology Products, NextGen Healthcare Information Systems, Inc. (Horsham, Pa.). "Now, when we go to ophthalmology meetings the questions are much more specific and the practice administrators are much better informed. This tells me they've done their due diligence, they have a comfort level with the improved systems that are now available and are about to make a purchase decision."
Messier estimates that 15% to 17% of the ophthalmology practices in the United States currently have EMR. He believes that 10 years from now that number could jump to 80%.
That is because vendors, including companies such as NextGen, MediNotes, Compulink, Medflow and OmniMD™, can now feel confident in telling practices that their investment in EMR — which can run up to $100,000 for a smaller practice and seven figures for a large practice — can pay for itself in as little as 12 to 18 months through the many efficiencies such systems offer to a practice.
For this article, Ophthalmology Management interviewed administrators and information technology (IT) experts from several practices that have recent experience in installing the new generation of EMR systems. All of these practices also made upgrading their electronic practice management systems part of an overall project. The article will attempt to answer the key questions that are on the minds of practice administrators and ophthalmologists currently contemplating the installation of EMR. In addition to examining why now may be the right time to consider implementing EMR, the article will provide guidance in the following areas:
? What is the best way to go about planning and implementing an EMR (or EMR/EPM) system?
? If you do intend to install an EMR system, should you also plan on upgrading your electronic practice management system as part of a single overall project?
? Should both your EMR and EPM systems be from the same vendor, or can you mix systems from different vendors if they can be designed into an integrated system?
Big Practice; Big Project
St. Luke's Cataract and Laser Institute, headquartered in Tarpon Springs, Fla., and started by James Gills, M.D., in 1968, today considers itself the largest cataract practice in the world. The full-service practice has four offices in the Tampa area, employing 12 ophthalmologists, seven optometrists and a staff of about 275 to treat a population demographic heavily skewed to retirees.
When Brad Houser was hired as administrator of the practice in 2003, one of his first priorities was to install an integrated EMR/EPM system.
"The electronic systems we had dated back to the 1980s. We needed to get up to speed," he says. "Given the size of the practice and the variety of services we provide, many patients see more than one physician. We needed a system that can track a wide range of information."
St. Luke's chose NextGen as its software vendor. NextGen says it is the industry leader in providing EMR systems to ophthalmology practices, accounting for an estimated 40% of all ophthalmology systems. It is also one of a handful of companies that can now offer larger practices an integrated, ophthalmology-specific EMR/EPM system that is customizable by the practice, capable of serving multiple locations, and able to directly access and capture data from diagnostic instruments. Smaller practices also now have a variety of EMR options, some of which allow the practice to interface its existing practice management system with an EMR from another vendor through a highly functional data-exchange protocol called HL7.
Bringing in a Consultant
Though St. Luke's is a large enough practice to have two full-time IT specialists on its staff, Houser also brought in independent consultant Ron Sterling, C.P.A., president of Sterling Solutions in Silver Spring, Md., to help with the overall installation and to pinpoint areas for staff training. Because of the magnitude of the project and the large size of the St. Luke's staff, an internal training team was formed so that training team members could be trained by NextGen, Sterling and the IT staff and then become trainers themselves.
"Undertaking an installation such as this is more than replacing pieces of paper with electronic records," says Sterling, who has served as an IT consultant for medical practices in 30 states. "You need to manage the project. You have to remember that the EMR vendor really only helps you to use its own product. The practice must make its own decisions as to how it's going to redesign the way it does business."
Sterling says many practices that switch to EMR underestimate its impact on the organization.
"Many don't understand the extent of the readjustment involved," he says. "You have to essentially rethink the organization. You have to supply your own project leadership because the vendor won't do that for you."
Sterling, who has written a book on EMR implementation called 2005 Guide to Buying and Implementing an Electronic Medical Record, says practices contemplating an EMR installation should have a detailed blueprint ready in advance for the entire project.
"You must know what you'll have at the finish," Sterling says. "Otherwise you can wind up with the wrong infrastructure, the wrong servers and the wrong hardware. EMR is much more complex than practice management because it functions in real time. Practices shouldn't even undertake EMR until they have a solid internal management structure that can support such a project and the project management expertise to carry it out."
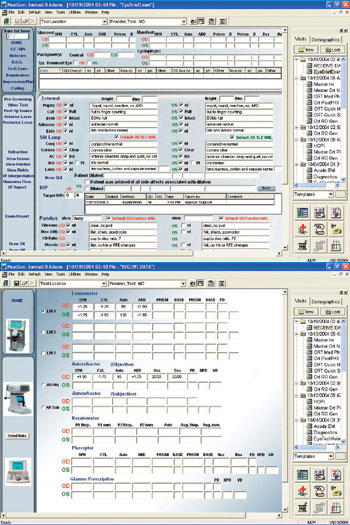
EMR developers offer ophthalmology-specific templates for easy information transfer. These NextGen templates show (top) a form for a basic eye exam and (bottom) a template to capture information directly from several diagnostic instruments.
 Two-Stage Installation Two-Stage Installation
For St. Luke's, Sterling and Houser decided on a two-stage installation, implementing the new EPM system during a slow period in the summer of 2004 and bringing the EMR system on line this summer.
Industry experts say this is the proper approach, as a new EPM system should be capable of running reliably for 4 to 6 months before being linked to the EMR system.
Houser says the practice is pleased with the performance of the EPM system after just 1 year in operation. He says concrete and objective measures of improvement include a significant drop in accounts receivables days outstanding, cash flow up 20% in 2005, although billings have increased by only 8%, and reduced errors on Medicare claims.
EMR developers offer ophthalmology-specific templates for easy information transfer. These NextGen templates show (top) a form for a basic eye exam and (bottom) a template to capture information directly from several diagnostic instruments.
"Overall, we've become more efficient in a number of areas, including billing, patient scheduling, patient flow and allocation of staff," says Houser. "We expect significant additional efficiencies to come from EMR. With the link to our EPM, the exam templates and the interfaces with our diagnostic equipment, the system will automatically feed information into patient records. We'll also communicate better between offices and be able to get patient records to our doctors instantly."
Houser says the keys to a smooth transition are extensive advance planning, dealing with a vendor who can provide a superior product and the use of an experienced independent consultant.
"You can't plan too much for something like this," says Houser. "Plan, plan, plan — but at some point you have to pull the trigger and do it."
A Three-Step Approach
The large Barnet Dulaney Perkins Eye Center, based in Phoenix, Ariz., has used a three-step plan to upgrade its EPM system and install EMR, says Executive Director Mark Rosenberg.
The statewide practice operates 10 ambulatory surgery centers and 14 offices. It employs 28 doctors and 320 staff, and encompasses all subspecialties of ophthalmology.
Also using NextGen as its software vendor, Barnet Dulaney Perkins upgraded its practice management system in 2002 and introduced EMR to only its refractive practice in 2003. Barnet Dulaney Perkins is now about to roll out EMR to the rest of the practice.
"We believed we would generate the strongest return on investment (ROI) by deploying EMR first in refractive, and that proved to be true," says Rosenberg. "ROI comes from the ability to harvest real-time data to optimize nomograms for LASIK surgery plans and to gather other important data to reduce our enhancement rate. By reducing enhancements, we have saved labor costs, supplies and royalty fees, and improved our risk management program."
Rosenberg says the practice wanted to choose a single vendor for both practice management and EMR because going that route provided more opportunity to integrate the system.
"With a single vendor, we won't have to worry about finger-pointing between vendors if a problem arises," he notes. "As a long-term thinker, I also wanted system we can use for the next 10 to 15 years and beyond, focusing on how our practice, the vendor's product and health care itself will evolve over that timeframe."
Rosenberg says all the values of EMR may not become apparent immediately and that not all of it can be quantified in dollars and cents.
"EMR gives you the ability to accumulate data, but the ROI is in using the data to optimize patient care," says Rosenberg. "For example, with EMR you can better track at-risk patients and dissatisfied patients. You can have a senior physician who's a glaucoma specialist and he can review reports on hundreds, or even thousands, of glaucoma patients and make recommendations to the treating physicians. EMR can be a teaching tool, an opportunity for peer review and a risk management tool as well."
Rosenberg says trying to set a date when the practice will have received full payback on its investment is short-sighted.
"You have to have a wider vision than just payback," he asserts. "It's possible that practices that don't embark on EMR will be out of business in 5 years. With mandates from payers and HIPAA it will be difficult for practices to meet the bar if they don't have electronic records systems for both EPM and EMR."
The Experienced User
William Constad, M.D., of Hudson Eye Physicians & Surgeons in Jersey City, N.J., is both an ophthalmologist and an IT specialist for his practice of seven physicians and 15 employees. He falls into the category of "early adopter" — a manager who's fascinated with advanced technology and who adopts it well before others in his profession are prepared to do so.
Dr. Constad wanted a single-vendor integrated IT solution, so he went with NextGen practice management and EMR about 5 years ago. The practice has been almost totally paperless since 2003.
"I wanted as little confusion as possible on the IT side," he notes. "You just don't want vendors pointing fingers at each other when there are problems. You can't have that in a doctor's office."
Dr. Constad wanted a great deal of flexibility in his system, so he designed his own ophthalmology-specific exam forms.
"I wanted to see things on the screen that made sense to me." he says.
Dr. Constad sees one role of EMR as a vehicle to generate efficiencies that help the bottom line while making life easier for doctors, staff and patients.
"The system has definitely helped to improve our percentage of clean claims," he says. "The system flags possible problems, and that results in fewer claims denied."
The system has also greatly reduced the number of staff hours devoted to billing.
"We now have one person doing the billing for the entire practice," says Dr. Constad. "Many practices of about our size have three billing people. And we can track our accounts receivable and days outstanding quickly."
Dr. Constad believes that most medical practices should place a higher percentage of their overall revenue into IT investment. He says having advanced technology can pay off in subtle ways.
"Patients comment favorably on the high-tech aspects of our office," he says. "They're impressed when we can give them their charts with the touch of a button. They also notice that the patient flow is smooth in our office. Our letters go out quickly. These are the little things that create satisfied patients and generate referrals."
EMR and EPM: Mix or Match
Dr. Constad understands that some practices that are ready to make the switch to EMR want to keep their existing EPM system because it is relatively new.
"If you have a practice management system that you bought 2 years ago, it's hard to justify another change now," he says. "It's not easy transferring information to a new system, especially financial information. And changing the practice management system will mean extra training for front-desk personnel."
Dr. Constad says to look at your current system and ask yourself, "Can I justify turning this over?" He says you might want to introduce EMR now and then switch the EPM in a couple of years.
Ron Sterling, the IT consultant, says that if your EPM is an old legacy system, it is probably preferable to replace it as part of your overall EMR implementation.
"Can you really go forward with an older practice management system? It might be an orphan system that no longer has vendor support. Remember, EMR will not make an old practice management system work better," he notes.
But if you can go forward with your existing EPM, Sterling says it is important to select an EMR system that can be compatible with your EPM.
"You can mix and match in some instances," Sterling advises. "If you have what I call a 'best-of-breed' practice management system, you may not have to change it. There are practice management systems available that are open to other vendors' EMR products."
The Case for Mixing
For example, Medflow, Inc. of Charlotte, N.C., produces a highly sophisticated and robust EMR system designed especially for ophthalmology practices. The company says most practices can retain their existing practice management system by interfacing with the Medflow EMR.
"We partner with a number of top practice management companies," says D. James Riggi, president of Medflow. "We can achieve very tight integration by linking our EMR to an existing practice management system. This is something we do routinely."
Charlotte Eye, Ear, Nose and Throat Associates in Charlotte, N.C., had a relatively new, top-of-the-line practice management system from IDX when it began to look into EMR in 2002.
"We explored every option," says Judith Bible, Au.d., COO of the practice, which employs 20 ophthalmologists at 10 locations, including a joint-venture surgery center. "We had initial concerns about integrating the systems, but we also saw advantages in keeping our existing best-of-breed practice management system. One major advantage was that we could focus our training effort on the clinical side. Another was that by retaining our practice management system we could keep better control of our accounts receivable during the transition."
Dr. Bible says IDX, EMR provider Medflow and the practice's strong IT team all worked together to interface the systems so that they could "talk" to each other.
"We've had EMR for about 22 months now and it interfaces with the practice management system seamlessly," she says. "IDX and Medflow have continued to work well together and we're happy with our decision."
Another well-established EMR company, MediNotes of Des Moines, Iowa, follows a similar business model. MediNotes has relationships with a number of best-of-breed practice management companies and can integrate its EMR with the practice management systems developed by these companies.
"IBM's new slogan 'Middleware is Everywhere', sums up the best-of-breed philosophy," says Don Schoen, CEO and president of MediNotes "Since the HL7 protocol for formatting, transmitting and receiving data has become the leading standard for data exchange in health care, the need for a suite of products from one vendor is no longer necessary, or for that matter desirable. Best-of-breed means that you don't have to compromise on software quality and functionality to have interoperable software in your office. You can carefully choose the best system for your needs in each category and combine them as you see fit.
"Our development team is 100% focused on creating and evolving the best electronic health record on the market," continues Schoen. "Today we have interfaces with nearly 40 practice management companies and many document managers, imaging software, appointment scheduling programs and laboratories. In fact, the majority of our 3,000 install sites have our Charting Plus product integrated with another software system and rely on it every day."
EMR has Arrived
Progressive practices and independent consultants agree that the more advanced and mature systems now available from the larger, established EMR vendors are going to result in more and more large and small practices transitioning to electronic records in the near future.
As the experts counsel, physician/owners and administrators considering making the switch must be ready to handle a major project that will affect almost every aspect of their practice. That means there must be a total, staff-wide commitment to doing the project — with the dollars allocated to doing it right.
"Don't try to do this on the cheap," cautions consultant Ron Sterling. "If you do, you could wind up with data security problems, too few software licenses and undersized servers, all of which will limit staff access to the EMR system."
The experts tell us that a well-planned and well-executed EMR implementation can move a practice forward in numerous ways: improving patient care, creating efficiencies, allowing for better allocation of staff, reducing transcription costs, saving space, eliminating paper and generally making life easier for doctors, staff and patients. Conversely, a poorly planned implementation can be costly and chaotic. The key to achieving the former and avoiding the latter is to do everything necessary to obtain the expertise that will enable the practice to make knowledgeable and informed decisions.
"If you're going to transition to EMR, you will need some people on board who really know what they're doing," concludes Ron Sterling.
Five Keys to Implementing EMR
In interviewing practice administrators, physicians, independent IT consultants and software company representatives who are involved in facilitating the switch from paper records to EMR, all agreed that the following five elements are critical in achieving a successful EMR implementation.
1. Have a stable organization. A practice should only begin seriously contemplating installation of EMR when it is financially healthy and has stable, solid leadership. Transitioning to EMR is one of the biggest projects that a practice will ever undertake. It is imperative that everyone in the practice is "on board" with the project and that there are no other major issues to deal with that could draw energy and resources away from the EMR installations.
2. Engage in sound planning. Planning for an EMR or EMR/EPM installation must be thorough and comprehensive, with particular attention paid to choices that need to be made in terms of infrastructure, hardware and software. Even if a practice has an in-house IT staff, hiring an experienced independent consultant early on who has been through many EMR installations is worth the money. The consultant can advise on purchase decisions, organize the extensive internal training effort that is required and provide the overall project management that ensures that the completed system will function as planned.
3. Provide adequate funding. Allocate enough money to conduct a first-rate EMR or EMR/EPM installation. This is one area in which going with the lowest bidder will probably cost a practice money in the long run. Choose a vendor that has a track record and that will be around to support the system 10 years from now. Scrimping on the installation budget can leave a practice with a less-than-robust system that will fail to perform as intended.
4. Have a vision. Growing practices should have a vision of what benefits the electronic system can deliver in both the short-term and the long-term. Make sure that the system is robust enough to keep up with the growth of the practice and meet future needs.
5. Have reasonable expectations about the return on the investment. Do not try to quantify every way that an investment in EMR or EMR/EPM can achieve payback. Some of the benefits, such as the number of staff hours saved on specific tasks, can be measured. However, other benefits can be more subtle and only become apparent over time. For example, many practices with EMR say patients are impressed with the speed and ease with which a high-tech office operates. This results in satisfied patients and referrals. Smaller practices considering EMR should recognize that although initial bottom-line savings may not be huge, the long-term benefits of having EMR may justify the cost.
Click here to see the Online Version at Opthalmology Management
|







